Designing AI for Mental Health Intake: Asking Less, Supporting More

A patient-facing AI intake assistant designed to reduce friction, protect emotional trust, and hand off to humans at the right moments.
Context
I worked on an AI patient-intake project for a regional U.S. behavioral healthcare provider, one of the largest mental health networks in its state.
The starting point was operational: long intake time, repetitive admin work, scheduling friction. Clinicians were spending close to 40% of every week on non-clinical admin.
But in mental health, the more useful question was not what AI could do. It was what AI should not do.
My Role
I joined as a UX consultant, leading conversation design, intake journey mapping, and human-AI handoff logic.
The Real Problem
The provider’s existing intake was mostly in-person or via phone. The goal was to bring that process online with AI.
The market standard for digital intake is a long form: patients answer everything up front, then learn at the end whether they qualify.
In mental health, that tradeoff is dangerous: the intake experience can either build trust early or break it before care begins.
Three Design Principles
Minimum Workflow before prompts
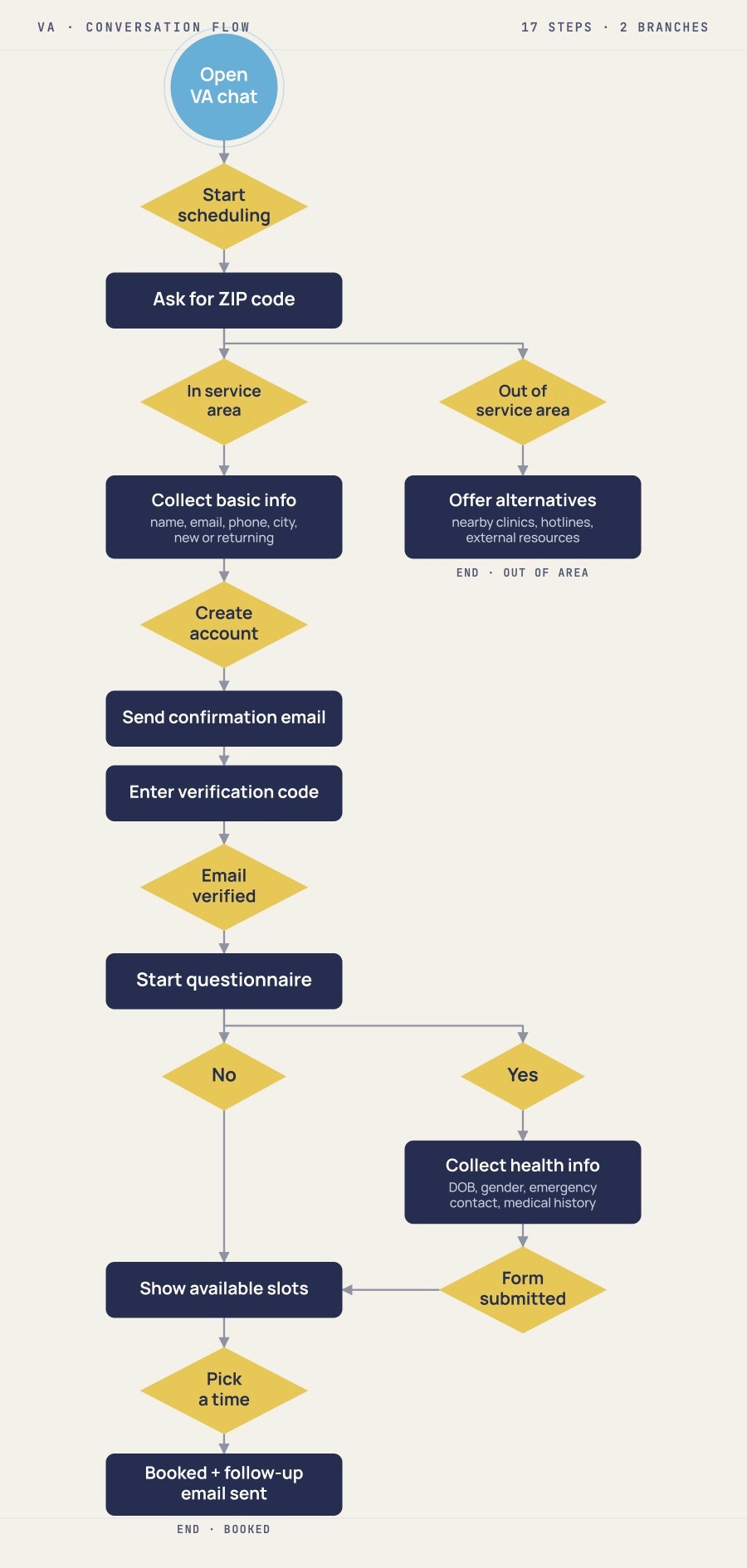
The new conversation flow asked the minimum at each step, before writing any prompts.
The assistant did not start with a long intake sequence. It first gathered just enough context to understand eligibility and next steps.
If the patient was not a match, the experience offered direct alternatives, such as community resources, support groups, or language services.
Information replaced rejection.
Emotional support as product logic
For patient-facing AI in mental health, tone is part of the product.
A scheduling assistant can create anxiety if it asks the wrong question or feels like a dead end.
The assistant’s tone had to acknowledge uncertainty, reduce anxiety, and make the patient feel guided rather than screened.
Human handoff by design
The assistant was not built to handle everything.
It could qualify, calm, inform, and schedule. But anything involving clinical judgment, sensitive disclosure, escalation, or diagnosis stayed with humans.
Each handoff had to be explicit, so patients knew when a person was about to take over.
What Changed
The redesign was projected to reduce intake time by 40%, with directional gains in patient satisfaction and appointment completion.
The bigger shift was less visible: the leadership conversation moved from “buy a tool” to “redesign the workflow first.”
What This Shows
Useful AI in mental health is less about automation and more about restraint. The work was not in choosing a model. It was in deciding what the assistant should leave alone.
That is the design judgment most AI projects skip. It is the same judgment the AI Fit Review brings to your business: what to buy, what to fix, and what to leave alone.